Prospects for accelerated fertility decline in
Africa
John
Cleland
John
Cleland is Professor Emeritus of Medical Demography at the London School of
Hygiene & Tropical Medicine. He is a former president of the International
Union for the Scientific Study of Population, a fellow of the British Academy
and received a CBE for services to social science.
John.Cleland@lshtm.ac.uk
–––––––––––––––––––––––––––––––––––––––––––
DOI: 10.3197/jps.2017.1.2.37
Licensing: This article is Open Access (CC BY 4.0).
How to Cite:
Cleland, J. 2016. 'Prospects for accelerated fertility decline in Africa '. The Journal of Population and Sustainability 1(2): 37–52.
https://doi.org/10.3197/jps.2017.1.2.37
–––––––––––––––––––––––––––––––––––––––––––
Abstract
The future size of world
population depends critically on what happens in sub-Saharan Africa, the one
remaining region with high fertility and rapid population growth. The United
Nations envisages a continuing slow pace of fertility change, from five births
per woman today to three by mid-century, in which case the population of the
region will increase by over one billion. However, an accelerated decline is
feasible, particularly in east Africa. The main grounds for optimism include
rising international concern and funding for family planning (after fifteen
years of neglect), and favourable shifts in the attitudes of political leaders
in Africa. The examples of Ethiopia and Rwanda show political will and
efficient programmes can stimulate rapid reproductive change.
Keywords: Africa; population projections;
fertility; desired family sizes; population policies.
Introduction
The
future of the world’s population depends on many factors that are impossible to
predict with certainty. A devastating pandemic is a distinct risk. The 1918 flu
pandemic is estimated to have killed about 4% of the world’s population. A
repetition today would imply the death of 280 million, a huge number but one
that represents only about four years of growth at current rates. Another
possibility that would have a profound impact on future population growth is a
substantial rise in China’s low birth rate in response to the ending of the
One-Child policy. But the biggest uncertainty is the future of fertility in
sub-Saharan Africa, the one remaining region with high birth rates and rapid
population growth. Compared with projections based on an assumption of a
continued gentle decline, an accelerated decline in fertility would reduce
Africa’s projected population size by 200 million by mid-century, rising to 800
million by the end of the century (Gerland, Biddlecom and Kantorova 2016).
The
central aim of this paper is to analyse the prospects for future fertility
change in sub-Saharan Africa. This will require an examination of past trends,
an attempt to understand the factors underlying the persistence of high
fertility and the conditions favourable to decline, and identification of
policies and programmes that can most effectively change the future course of
childbearing.
Projected population growth,
2015-2050
Table
1 shows the most recent medium (ie most likely) population projections up until
mid-century published in 2015 by the United Nations Population Division.
Longer-term projections exist but are highly speculative because they have to
make assumptions about the childbearing of individuals not yet born. Over a
horizon of a few decades, UN projections have a good record of predictive
validity at global and regional levels. While by no means immutable, they
deserve to be taken seriously.
Table
1 shows an expected increase in global population of 2.4 billion between 2015
and 2050. The growth comes very largely from two regions, Asia with an extra
870 million and sub-Saharan Africa with 1.2 billion. The proportionate
increases in these two regions, however, are very different. In Asia, the
projected increase is a mere 20%, about the same as expected in northern
America, largely because of assumptions of continuing in-migration, and lower
than in Latin America or north Africa. The large increment of 870 million in
Asia is mainly a reflection of that region’s huge base population size. By
contrast, the population of sub-Saharan Africa is projected to more than double
in size, an increase of 120%. Whatever happens in regions other than Asia and
sub-Saharan Africa will make precious little difference to the global total in
mid-century. Differential growth has had and will continue to have a profound
effect on the regional balance of population. In 1950, sub-Saharan Africa
accounted for only 7% of world population. By 2050, this fraction will likely
rise to 22%. Over the same 100 years, Europe’s contribution is the exact mirror
opposite, a decline from 22% to 7%.
Table 1: Population Growth,
2015-2050, by region
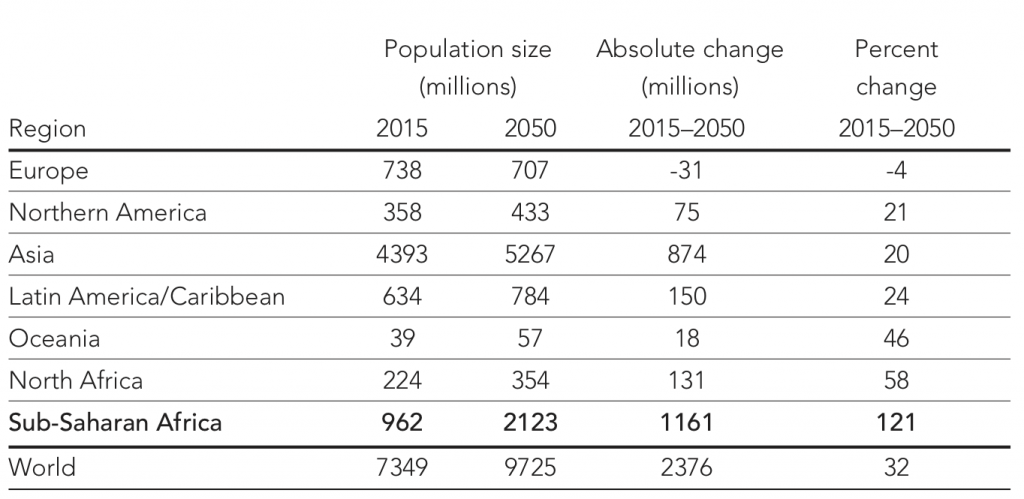
Source: United Nations. 2015
World Population Prospects: The 2015 Revision
The main drivers of population growth are fertility and age
structure: the higher the proportion of population in the reproductive age
span, the higher will be the birth rate at the same level of childbearing per
woman. Figure 1 shows past and projected fertility for the same six regions as
in Table 1. In the 1950s, fertility in the four poorer regions was similar, in
the range of six to seven births per woman. In Asia and Latin America, sharp
declines started in the 1960s and fertility is now close to two births per
woman, the replacement level that in the long term ensures population
stability. Population growth continues mainly because of a conducive age
structure. In its projections the United Nations assumes a continuing fall in
fertility to below replacement. In the Arab states of north Africa the drop in
childbearing also started in the 1960s and the United Nations assumes a
continuing fertility decline, from a little over three births today to close to
replacement by mid-century. In sub-Saharan Africa, decline started later and
proceeded at a slower pace than elsewhere. The UN assumes that the gentle
decline will continue from the current level of about five to about three births
by 2050.
Figure 1: Trend of total
fertility rate by world region, 1950-2050 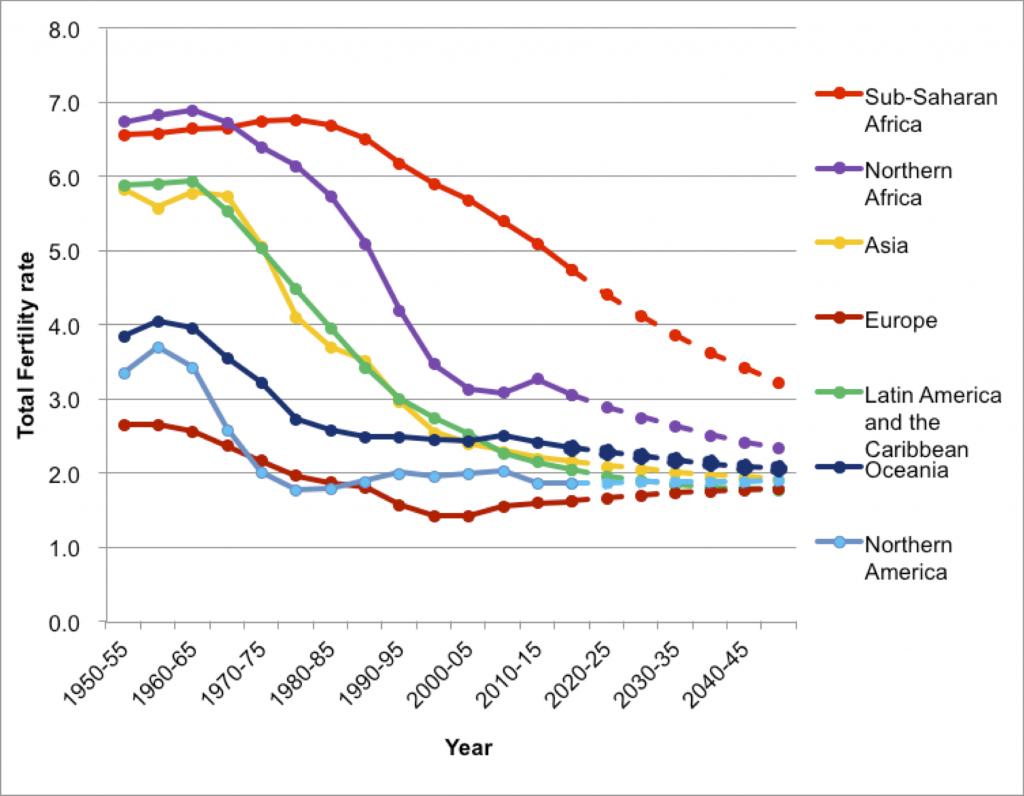 Source:
United Nations.2015 World Population Prospects: The 2015 Revision
Source:
United Nations.2015 World Population Prospects: The 2015 Revision
Of
course, these regional averages disguise country variations. In Asia, the main
exceptions to prevailing low fertility and population growth are Afghanistan,
Iraq and Yemen where the child-bearing level is still around four births.
Fertility also remains above three in Pakistan’s substantial population. In
sub-Saharan Africa, fertility ranges from close to replacement in the Republic
of South Africa to over seven births per woman in Niger. This variability is
expressed in Figure 2 in terms of projected percent increase in population
between 2015 and 2050. Figure 2 makes clear that most countries in Africa are
expected to experience a doubling of population, or more, in the next 35 years.
Only 11 of the 46 countries are projected to grow by appreciably less than
100%.
Figure 2: Percent increase in
population between 2015 and 2050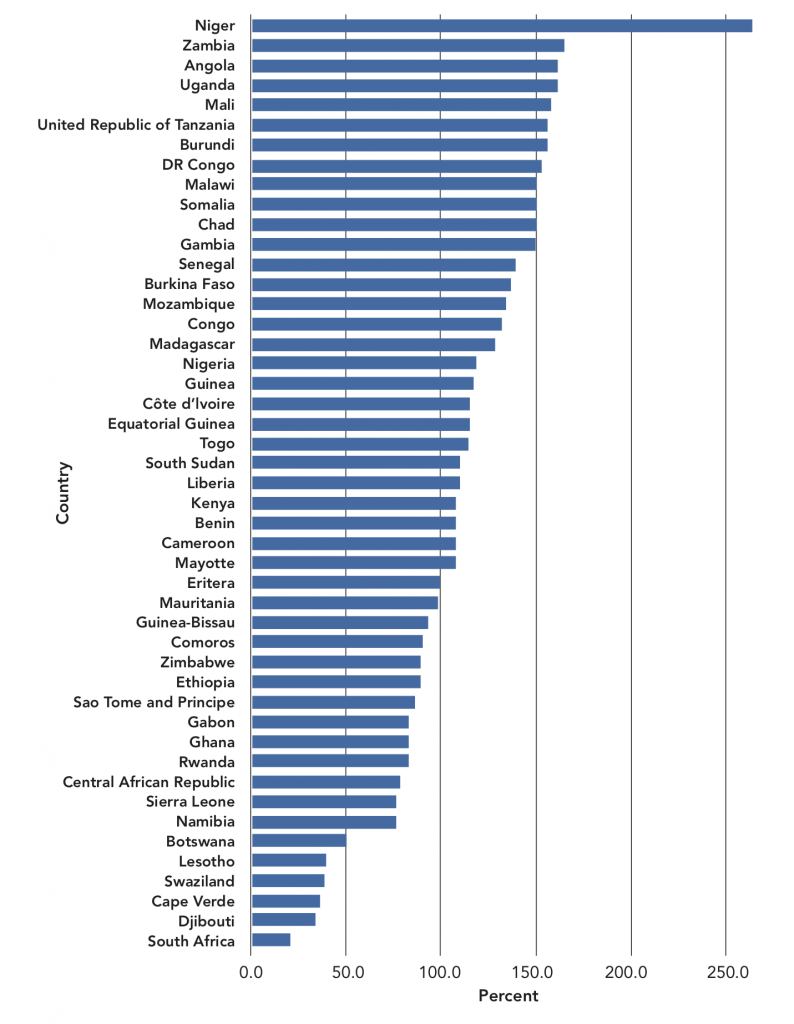
Source: United Nations.2015
World Population Prospects: The 2015 Revision
Niger
with a projected increase of 250%, from 20 million to 72 million demands
special consideration. This is a relatively rare example of a projection that
makes no sense. Niger has a very fragile environment, highly susceptible to
climate change, and suffers periodic food crises. It is impossible to envisage
that the country can support such a growth in population, even at the most
basic standards, or that international food relief can come indefinitely to the
rescue on such a massive scale. The inevitable resolution will be mass
migration, mostly to neighbouring countries. Whether this can happen without
major strife is one of the great uncertainties but the topic is so politically
sensitive that it is ignored in international discourse. Niger is only an extreme
example of a Malthusian crisis that will affect the whole of the Sahel, the
strip of arid and semi-arid land stretching from the Atlantic to the Horn of
Africa (Potts, Henderson and Campbell 2013). As shown in Figure 2, population
projections for Mali and Chad are also very high.
Explanations for the slow
fertility decline in sub-Saharan Africa
What
distinguishes African reproductive systems most clearly from those in other
parts of the world is the stated desire for many children, expressed by both
women and men in countless surveys. The earliest surveys in Asia and Latin
America, conducted in the late 1950s and 1960s typically showed that most
couples wanted to have two to four children; many women in their 30s wanted to
stop childbearing altogether. In sub-Saharan Africa, desired family sizes were
(and remain) much larger and fewer women wanted to stop. For instance, World
Fertility Surveys, conducted in the 1970s and early 1980s, show that desired
sizes among young women in seven African countries ranged from 5.2 in Ghana to
8.3 in Senegal. By contrast, in only one (Syria) of 14 Asian and Pacific
countries did the mean desired size exceed five children. In 13 Latin American
and Caribbean countries, the highest desired size was 3.8 in Mexico
(Lightbourne 1987).
What
accounts for this huge difference in attitudes towards childbearing? Answers
can be sought in evolutionary history. Homo sapiens evolved in Africa, facilitating the
co-evolution of a uniquely wide range of parasitic diseases, leading to
exceptionally high mortality. Africa’s population is characterised by a mosaic
of different ethnicities with rather little historical evidence of large
empires that could impose eras of peaceful co-existence. Mortality was thus
further raised by incessant raiding and warfare between different tribes. These
two factors go a long way to explaining Africa’s small population size until
recently. They may also account for reproductive attitudes. Survival of the
group depended on a high birth rate and, in particular, on the ready
availability of young men to protect against aggressive neighbours.
The
speculations in the preceding paragraph are consistent with more commonly
expressed explanations. John Caldwell has argued forcefully that features of
social organisation, underpinned by traditional African religion, served to
engender and sustain pronatalism (Caldwell and Caldwell 1987; Caldwell,
Orubuloye, and Caldwell 1992). Drawing on anthropology and his own extensive
field studies in Nigeria, Caldwell viewed the extended lineage, rather than the
nuclear family, as the key feature of social organisation. The lineage includes
both the living and the dead. The dead retain their individuality for as long
as they are specifically remembered and may be reborn into the lineage. The imperative
for both living and dead is survival of the lineage. Reproduction is enforced
with spiritual power and reproductive failure is interpreted as ancestral
disapproval.
The
dominance of the lineage also has more prosaic economic implications. Mortality
decline invariably precedes drops in fertility and, as a consequence, the
number of children who survive to adulthood rises. Whereas in Asia, the burden
of rearing an increasing number of surviving children fell directly on the
nuclear parents, in Africa the burden is diffused among relatives. More
affluent lineage members are under an obligation to help those less fortunate
with, for example, school fees. Child fostering is common. A related factor
concerns land tenure in much of Africa, which is controlled by communities and
allocated to individuals according to need. These features are likely to delay
a fertility response to improving survival.
Other
commentators have sought to account for the slow decline in fertility more
straightforwardly in terms of low socio-economic development. All the familiar
indicators—life expectancy, GDP per head, percent urban and educational level—
are less favourable in Africa than elsewhere. A recent examination suggest that
the level of development at the start of the African fertility transition in
the 1990s was lower than in other developing regions at the start of their
transition in the 1970s (Bongaarts 2016). Nevertheless, at the same level of
development, fertility in African countries is about one birth higher than
elsewhere. In other words, there is a unique “Africa” effect on childbearing.
Yet a
further explanation is the relative lack of firm policies and programmes to
reduce rapid population growth by promotion of contraception. Opinion is
divided about the effectiveness of family planning programmes to reduce
fertility. Most economists are sceptical and view demand for smaller families
stemming from modernisation as the overridingly important factor. But they
ignore the fact that contraceptive practice represents a radical innovation
that concerns core features of human life—sex and procreation. Like most such
innovations, contraception is often greeted with deep suspicion and anxiety and
sometimes with outright hostility. Information and educational efforts, together
with family planning services, organised by governments or large
non-governmental organisations, can allay suspicion and subdue opposition and
thereby hasten mass adoption of contraception and fertility decline. Strong
government actions were a major influence on fertility transition in Asia,
though less so in Latin America where initiatives were spearheaded by
non-government organisations such as Profamilia in Colombia and Bemfam in
Brazil.
Until
recently, the attitude of African political leaders to the idea of fertility
reduction and curbing population growth has been lukewarm or hostile, no doubt
in part because of the perception by leaders that most citizens wanted large
families (May 2016). Few governments have launched major family planning initiatives.
The main exceptions have been South Africa under the Apartheid regime, Rhodesia
(now Zimbabwe) under the illegal Smith regime and Kenya in the 1980s under
President Moi; it is no coincidence that these three countries have been at the
forefront of reproductive change in Africa.
Prospects for accelerated
fertility declines
The
UN medium projections, thus far, have been used to portray the most likely
future for Africa’s fertility trend and population growth. But, as already
mentioned, they are not set in stone. In this section, future fertility
prospects are assessed in three very different ways: trends in the desire to
stop childbearing; the reproduction of the best educated; and the lessons from
two countries that have achieved recent rapid declines.
Desire to stop childbearing
In
Asia, Latin America, and north Africa, the fall in childbearing was dominated
by family size limitation. Couples, typically in their early 30s, having had a
few children, decided that they wanted no more and adopted contraception to
achieve this desire. Some evidence suggests that the African fertility
transition is taking, and will continue to take, a very different form. Rather
than contemplating a permanent cessation of childbearing, it is suggested that
couples will postpone births and reduce ultimate family size by very long
inter-birth intervals (Moultrie, Sayi and Timaeus 2012). Such behaviour is
consistent with a large and convincing body of evidence that wide birth spacing
has long been valued in Africa and indeed has an important role in enhancing
child growth and survival. Historically it was achieved by prolonged postnatal
sexual abstinence.
Nevertheless,
it seems unlikely that low fertility will be achieved in Africa solely by
postponement and spacing. Women start families at an early age and, even with
average inter-birth intervals of 48 months, five children can be achieved with
ease. It is also telling that prospective studies in Nigeria, Ghana, Malawi and
work in progress in Kenya show that women or couples who state at baseline that
they want no more children do indeed achieve lower fertility in the subsequent
two or three years than those who state a desire for more children at some time
in the future. In rural North Malawi, for instance, 33% of women who stated
that they wanted no more children gave birth or became pregnant within the next
three years compared with 55% of those who wished to delay the next child by
three or more years and 63% of those who wanted a child within three years
(Machiyama et al. 2015). The proportion of those wishing to stop who
nevertheless became pregnant may seem large but similar results have been
obtained in Asia and north Africa and many possible explanations can be found:
change of preference; contrary desires of the husband; and contraceptive
failure, discontinuation or avoidance. The significance of the Malawi results
is that the family size limitation appears to provide a more compelling motive
for pregnancy-avoidance than postponement. Perhaps, after all, the pattern of African
reproductive decline will not be so different from that in other regions.
To
the extent that the spread of family size limitation is essential for the goal
of low fertility, it becomes relevant to examine trends in the desire to stop
having any more children. Table 2 shows these trends for women who already have
three surviving children. The choice of three children is in part arbitrary but
also justifiable on the grounds that low fertility is unlikely until a large
fraction of couples are content to have a small family of three or fewer
offspring. Countries with at least four Demographic and Health Surveys have
been chosen for this analysis.
Table 2: Among women with three
living children, percentage who want no more
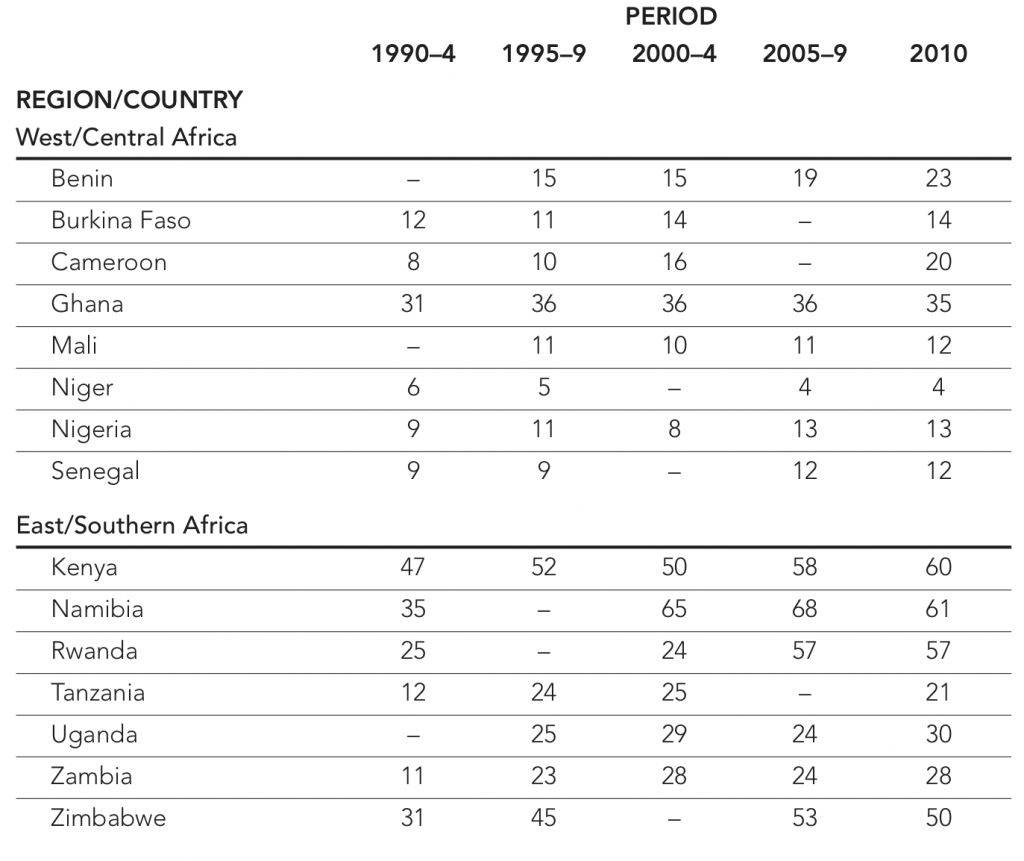
The
trends for west and central Africa are depressing in terms of prospects for
decline. In most countries, only a small minority of women wish to stop
childbearing after three children and trends over the past 20 years are modest.
Cameroon is a partial exception, with an increase from 8% to 20% between the
early 1990s and recent years. Ghana, the forerunner of fertility decline in
this sub-region, has a much larger proportion wishing to cease childbearing
though little change has occurred in the past two decades.
In
east and southern Africa, the impression is very different. In four of the
seven countries, half or more of women with three children express contentment
with this number. The exceptions are Tanzania, Uganda and Zambia. In both
Tanzania and Zambia, a sharp rise from around 12 to 24% is apparent in the
1990s but there has been little further change since then.
Kenya
is a particularly interesting case. In the World Fertility Survey of 1979-80,
only 16% of all married women wanted no more children but within a decade this
proportion had swelled to 49%. This decade saw the implementation of a vigorous
family planning programme, with a strong informational and educational
component, led by President Moi and Vice-President Kibaki, and a surge in
contraceptive adoption. This sequence suggests that reproductive aspirations
can be abruptly de-stabilised by the advent of reproductive choice. Something
similar may have occurred in Rwanda. In this country the dramatic rise in the
percent wishing to stop at three children in the first decade of this century
coincided with a major re-invigoration of family planning under the auspices of
President Kagame. However, puzzles remain. In Zambia, use of a modern
contraceptive method rose sharply from about 20% in 2000 to 45% in 2013, about
the same level of use as in Rwanda, but without the revolution in reproductive
attitudes.
The
broad conclusion from this examination of reproductive preferences is that the
idea of family size limitation has taken root in much of east and southern
Africa and the prospects of further declines look bright. The opposite applies
to west and central Africa.
Fertility among well educated
women
The
reason for attempting to discern the future by examining current levels of
childbearing among well educated women is that they are usually in the vanguard
of change. Contraceptive adoption and a fall in fertility usually starts in
privileged strata before diffusing more widely. Thus the reproduction of women
with secondary or higher schooling in Africa may be a guide to behaviour in the
total population in the next couple of decades.
A
total of 13 west or central Africa countries have conducted Demographic and
Health Surveys, or similar, in 2010 or more recently. The percent of women aged
15-49 years with some secondary or higher education ranges from 9% in Niger to
63% in Ghana, with a mean of 29%. Among this group, the lowest fertility is
recorded in Cote d’Ivoire at 2.8 births. Fertility of over 4.0 is apparent in
Niger (5.0), Mali (4.6), Nigeria (4.5) and Gambia (4.5). The mean for all 13
countries is 3.8.
In
east and southern Africa the percent of well educated women ranges from 11% in
Ethiopia to 73% in Zimbabwe, with a mean among 11 countries of 31%. In this
group the highest fertility is found in Burundi (4.6) and Uganda (4.5) and the
lowest in Ethiopia (1.9). Mean fertility is 3.5 births.
Several
observations may be made on the basis of this simple exploration. First,
achievement of secondary schooling does not automatically translate into low
fertility as evidenced in seven of these 24 countries. Second, the large
east-west divide seen in Table 2 largely disappears when attention is focussed
on behaviour of the well educated. The level of women’s education is similar
and, while fertility, on average, is lower in the east than the west, the
difference is small. Third, the indications for future fertility decline tend
to be positive. Close to one-third of women of reproductive age have received
secondary or higher schooling and their fertility is currently not much above
three births, compared with about five for all women. Secondary school
enrolments are destined to increase in the future and, more importantly, the
less well educated are likely to follow the reproductive path of their better
educated counterparts.
The lessons of success
Two
countries, Ethiopia and Rwanda, have experienced remarkably sharp recent
fertility declines. What can be learnt from these successes?
Ethiopia’s
population is estimated to be about 100 million, the second most populous
country in sub-Saharan Africa. Despite rapid growth in GDP in the past 10
years, it remains one of the world’s poorest countries and is the world’s
largest recipient of international food aid. School enrolments have improved
but adult educational levels are low. Half of women of reproductive age have
received no schooling and, as shown above, the percentage with secondary
schooling is exceptionally low.
Despite
these disadvantages, the country has achieved an impressive degree of
demographic modernisation. For instance, life expectancy improved by close to
16 years between 1990 and 2013, whereas the gain for Africa as a whole was only
about six years. Similarly, fertility fell from seven births per woman in the
early 1990s to 4.6 births in 2010-15, a drop of 35% compared with a drop over
the same period of 18% for the entire region.
Strong
policies and programmes can take much of the credit for these stunning
achievements (Halperin 2014). The 1993 population policy set explicitly
demographic goals of reducing fertility to four births and raising
contraceptive use to 44% by 2015. In 2004, the abortion law was liberalised. A
cadre of over 30,000 mainly female community-based health and family planning
workers was trained for one year and posted back to their own localities. One
lesson from Ethiopia, like that of Bangladesh in the 1980s, is that major
progress towards low mortality and fertility can be made in the absence of
broad socio-economic development given political will and programmatic
efficiency.
Rwanda,
a much smaller and more densely populated country than Ethiopia, is placed at
position 163 out of 188 on the human development index, the same as Uganda but
slightly higher than Ethiopia at position 174. The country adopted a
pronatalist stance in the aftermath of the genocide but in 2003, the policy
changed to the goal of reducing population growth and, as in Ethiopia, a strong
emphasis was given to outreach family planning services. Between 2005 and
2014/5, the percent of married women using a modern contraceptive method rose
from 10 to 48% and fertility fell from six to a little over four births per
woman, an astonishingly rapid transformation.
The
key lesson from Ethiopia and Rwanda appears to be that determined government
initiatives can bring about rapid reproductive change as part of a wider agenda
of health improvements, educational expansion and economic vibrancy. Both
political regimes run relatively efficient administrations that are capable of
mass mobilisation and implementation of effective nationwide programmes. Both
are autocratic, with little tolerance for opposition, and it remains uncertain
whether political evolution towards greater inclusiveness and freedom of
expression will occur. The civil insurrection in Ethiopia in October 2016 is
certainly a warning sign that a more inclusive approach is needed.
Nevertheless, the experience of these two countries is relevant to the more
secure and competent regimes in Africa.
Discussion
As
stated at the outset of this paper the future size of the world’s population
depends largely on what happens to fertility in sub-Saharan Africa. The skilled
and experienced team of demographers at the UN Population Division think that
the pace of decline will continue to be as gentle as in the past. They may well
be correct, particularly for west Africa. Some of the evidence reviewed here,
however, suggests that sharper declines could be achieved. In addition, rapid
urbanisation is expected in Africa. Though this will result in a proliferation
of slum populations, fertility is markedly lower in urban slums than in rural
areas and thus rural-urban migration will favour drops in childbearing. Further
expansion of secondary schooling will also accelerate the pace of change, as
will increased exposure to mass media.
Developments
in the application of birth control technologies are a further relevant factor.
Hitherto, injectable contraception has been dominant. Though highly effective,
this type of method requires re-supply every two or three months.
Discontinuation because of side effects and health concerns is common and
switching to an alternative method is low. The link between contraception and
pregnancy-avoidance is thus weakened. In response, there is a new emphasis on
the promotion of long-acting reversible methods, intra-uterine devices and
implants, which have much lower rates of discontinuation than injectables,
perhaps because stopping requires a conscious decision to remove the device.
Use of implants, but not IUDs, is now rising rapidly in many countries. The
proliferation of medical abortion products, often available illegally across
the counter in medical stores, may already be having an effect on childbearing,
particularly among sexually active single young women for whom the stigma of
abortion is less than the shame and threat to prospects of motherhood
(Johnson-Hanks 2002).
The
most compelling grounds for optimism concerns politics, both international and
domestic. Just as the fertility transition was starting in Africa in the early
1990s, international concerns about high fertility and rapid population growth
waned. At the 1994 Cairo conference on population and development, the agenda
of population control was swept aside and replaced by a broader vision of
women’s reproductive health, rights and empowerment. Subsequently, the
desirability of curbing population growth, and even the word “contraception”
disappeared from international discourse. In Africa, family planning funding
was diverted to a new emergency, HIV. As high fertility and rapid population
growth jeopardises employment prospects, food security, improvement of human
capital and the environment, Africa’s long term prospects were severely damaged
by the new international consensus.
The
pendulum of international opinion has now swung back. The worst of the HIV
pandemic is over, new concerns have arisen about the world’s ability to feed a
growing population without further severe environmental damage, and the huge
surge in Africa’s population has raised alarms about mass migration from
poverty and hunger. In 2012, the London Family Planning Summit pledged to reach
an extra 120 million women with affordable contraception by 2020. Funding has
increased and the reluctance to talk openly about the subject has abated.
This
change at the international level will achieve little without changes at
national governmental level. Here also, positive developments are apparent. The
concept of a “demographic dividend” has traction among African politicians and
economists. This dividend, or boost to living standards, arises when the
falling fertility brings in its wake a rise in the ratio of adult workers to
dependent infants and children. Econometric evidence suggest that this change
in age structure made a large contribution to rapid improvements in income per
head in east Asia. This prospect is appealing to African elites. Poverty
reduction is a universal goal and the narrative of the demographic dividend
neatly circumvents explicit mention of curbing population growth, though, of
course, it will have exactly this effect. President Museveni of Uganda,
historically an opponent of family planning promotion, has been convinced and
other leaders are showing similar signs, spurred on by endorsements from the
World Bank and IMF (May 2016). We are entering an era when political will and
(hopefully) international funding may act in concert to accelerate reproductive
change. The re-imposition by President Trump in January 2017 of the global GAG
rule that prevents US funding of any non-government organisation that in any way
promotes or facilitates access to abortion is a backward step but in the past
this restriction has not made a decisive difference to overall funding for
family planning, in part because other donors made good the deficit.
References
Bongaarts,
J. 2016. Africa’s unique fertility transition. Population and Development Review DOI:10.1111/J.1728-4457.2016.00164.X
Caldwell,
JC and Caldwell P. 1987. The cultural context of high fertility in sub-Saharan
Africa. Population and Development Review 13(3):409-437
Caldwell
JC, Orubuloye IO, and Caldwell P. 1992. Fertility decline in Africa: A new type
of transition? Population and Development
Review 18(2):211-242
Gerland
P, Biddlecom A and Kantorova V 2016. Patterns of fertility decline and the impact
of alternative scenarios of future fertility change in sub-Saharan Africa.
Population and Development Review DOI:10.1111/padr.12011
Halperin
D. 2014. Scaling up of family planning in low-income countries: lessons from
Ethiopia. Lancet 383:1264-67
Johnson-Hanks
J. 2002. The lesser shame: abortion among educated women in southern Cameroon. Social Science and Medicine 1337-1349
Lightbourne
RE 1987. Reproductive preferences and behaviour. In Cleland J and C Scott (eds) The World Fertility Survey: An Assessment. Oxford: Oxford University Press.
pp.838-861.
Machiyama
K et al. 2015. An assessment of childbearing preferences in Northern Malawi. Studies in Family Planning 46(2):161-176
May
J. 2016. The politics of family planning policies and programs in sub-Saharan
Africa. Population and Development
Review DOI:10.1111/j.1728-4457.2016.00166.x
Moultrie
T, Sayi T and Timaeus I 2012. Birth intervals, postponement and fertility
decline in Africa: A new type of transition. Population Studies66(3):241-258
Potts
M, Henderson C, Campbell M. 2013. The Sahel: A Malthusian challenge. Environmental Resource Economics 55:501-512.